Stem cell treatment for colitis
Colitis encompasses inflammatory conditions of the colon, including ulcerative colitis and ischemic or infectious colitis. Stem cell–based therapies are being explored as potential options to modulate inflammation, promote mucosal healing, and restore intestinal homeostasis. Current research remains in early phases, and treatment decisions should be guided by qualified healthcare professionals and established clinical guidelines.
Overview
Stem cell therapy aims to harness the regenerative and immunomodulatory properties of various cell types to address the underlying inflammation and tissue damage in colitis. Investigations focus on approaches such as mesenchymal stem cells (MSCs), hematopoietic stem cells, and other multipotent or progenitor cell populations. Preclinical and early clinical data suggest potential benefits in reducing inflammatory activity and supporting epithelial repair, though evidence varies by condition and study design.
Mechanisms of action
- Immunomodulation: Stem cells can alter cytokine profiles and dampen excessive inflammatory responses.
- Tissue repair: Secretion of growth factors supports epithelial regeneration and vascularization.
- Barrier function: Restoration of the mucosal barrier helps prevent further injury and infection.
- Microenvironment modulation: Stem cells may influence the local tissue milieu to favor healing.
Types of stem cells under study
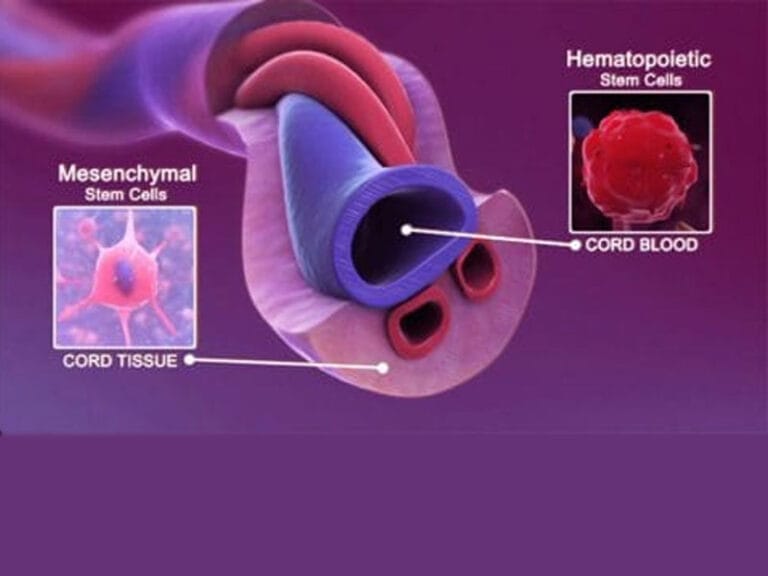
- Mesenchymal stem cells (MSCs): Derived from bone marrow, adipose tissue, umbilical cord, or dental pulp, studied for anti-inflammatory and reparative effects.
- Hematopoietic stem cells (HSCs): Explored in certain contexts related to immune system modulation.
- Induced pluripotent stem cells (iPSCs): Investigational for personalized approaches and disease modeling.
- Endothelial progenitor cells: Investigated for supporting vascular repair in damaged mucosa.
Evidence and clinical trials
- Early-stage trials have reported improvements in clinical symptoms and quality of life for some patients with ulcerative colitis, particularly with MSC-based therapies.
- Results are heterogeneous; some studies show modest benefit, while others indicate limited or no additional advantage beyond standard therapies.
- Safety profiles have generally been favorable in many trials, though longer-term follow-up and larger randomized studies are necessary to establish efficacy and optimal treatment parameters.
Administration and protocol considerations
- Delivery routes: Intravenous infusion is common for systemic effects; local delivery to the affected colon has also been explored in specialized settings.
- Dosing and frequency: Investigational protocols vary; optimizing cell dose, frequency, and duration remains an active area of research.
- Patient selection: Candidates often include individuals with moderate to severe disease refractory to conventional therapies, after careful risk-benefit assessment.
- Concomitant therapies: Stem cell treatment is typically considered in the context of ongoing standard-of-care regimens, with close monitoring for interactions and complications.
Safety and risks
- Common considerations: Infection risk, immune reactions, and potential for abnormal tissue growth or unintended differentiation.
- Long-term safety: Requires ongoing surveillance to detect delayed adverse events, including malignancy risk in some stem cell contexts.
- Regulatory status: Availability and approval vary by country and depend on adherence to clinical trial frameworks or approved indications.
Practical considerations for patients
- Consultation: Thorough discussion with gastroenterology and stem cell specialists to evaluate suitability and alternatives.
- Trial availability: Access may be limited to participating clinical trials or accredited centers offering experimental therapies.
- Expectations: Stem cell therapies are not universally curative and should be viewed as prospective options within a broader treatment plan.
Conclusion
Stem cell–based therapies for colitis represent a promising area of research with the potential to complement existing treatments. While encouraging signals exist from early studies, robust evidence from large, well-designed trials is required to define efficacy, safety, and optimal therapeutic protocols. Patients should pursue informed discussions with their healthcare teams to determine the most appropriate course of action based on current guidelines and individual medical circumstances.
j